The genetic risk of hip dysplasia cannot be altered by environmental measures. A dog either has a hereditary predisposition or it does not. Environmental management can reduce joint laxity in predisposed dogs but cannot change the underlying hereditary risk.
Hip dysplasia (HD) is a developmental disorder in which the femoral head and the acetabulum fail to develop in optimal congruence. Puppies are typically born with normal hips, but the joint may develop abnormally during growth if passive hip laxity is present. This instability leads, over time, to abnormal loading, microtrauma, and the development of osteoarthritis. HD is multifactorial. Many genes contribute to the risk, and environmental factors strongly influence whether a genetic predisposition becomes clinically apparent. Rapid growth, high energy intake, excess bodyweight, slippery surfaces and heavy physical strain during early life increase the risk, whereas lean body condition and controlled activity can reduce the severity.
The fundamental mechanism in HD is joint laxity early in life. When the hip joint lacks adequate stability, the femoral head moves slightly out of position during motion. This causes abnormal loading of the cartilage, inflammatory responses, and gradual remodelling of bone. Osteoarthritis is therefore a secondary consequence of long-standing instability, not the primary cause of HD. Modern research shows that the degree of passive laxity early in life is the best predictor of future risk, which is why methods that measure laxity directly are increasingly emphasised.
Traditional hip-extended radiography may underestimate passive hip laxity. Muscle tone can artificially stabilise the joint, the position does not represent normal loading, and young dogs often lack secondary osseous changes. A dog may therefore appear radiographically "normal" while still having measurable laxity. This is particularly relevant in muscular breeds such as the Staffordshire Bull Terrier. Different breeds have varying genetic backgrounds, biomechanical properties and selection histories, which lead to differences in HD prevalence and expression.
It is important to emphasise that the genetic risk of hip dysplasia cannot be altered by environmental measures. A dog either has a hereditary predisposition for HD or it does not. A dog without such a predisposition will not develop hereditary HD regardless of feeding, exercise or environmental conditions. In dogs that do carry a genetic predisposition, good environmental management can reduce the degree of joint laxity and thereby lower the risk of future problems, but it cannot change the underlying hereditary risk.
Radiographic findings can never reliably distinguish between what is caused by genetics and what is the result of environment, injury or growth conditions. The radiograph only describes the state of the hip joint at the time of examination — it does not reveal whether the changes are hereditary or environmentally induced.
Norwegian studies show that only a minority of dogs with mild or moderate HD experience clear daily-life limitations, but that dogs with radiographic HD, on average, have a higher risk of load-related issues than dogs with normal hip scores. However, this reflects the individual dog's condition, not whether the changes are inherited.
Diagnostic Systems
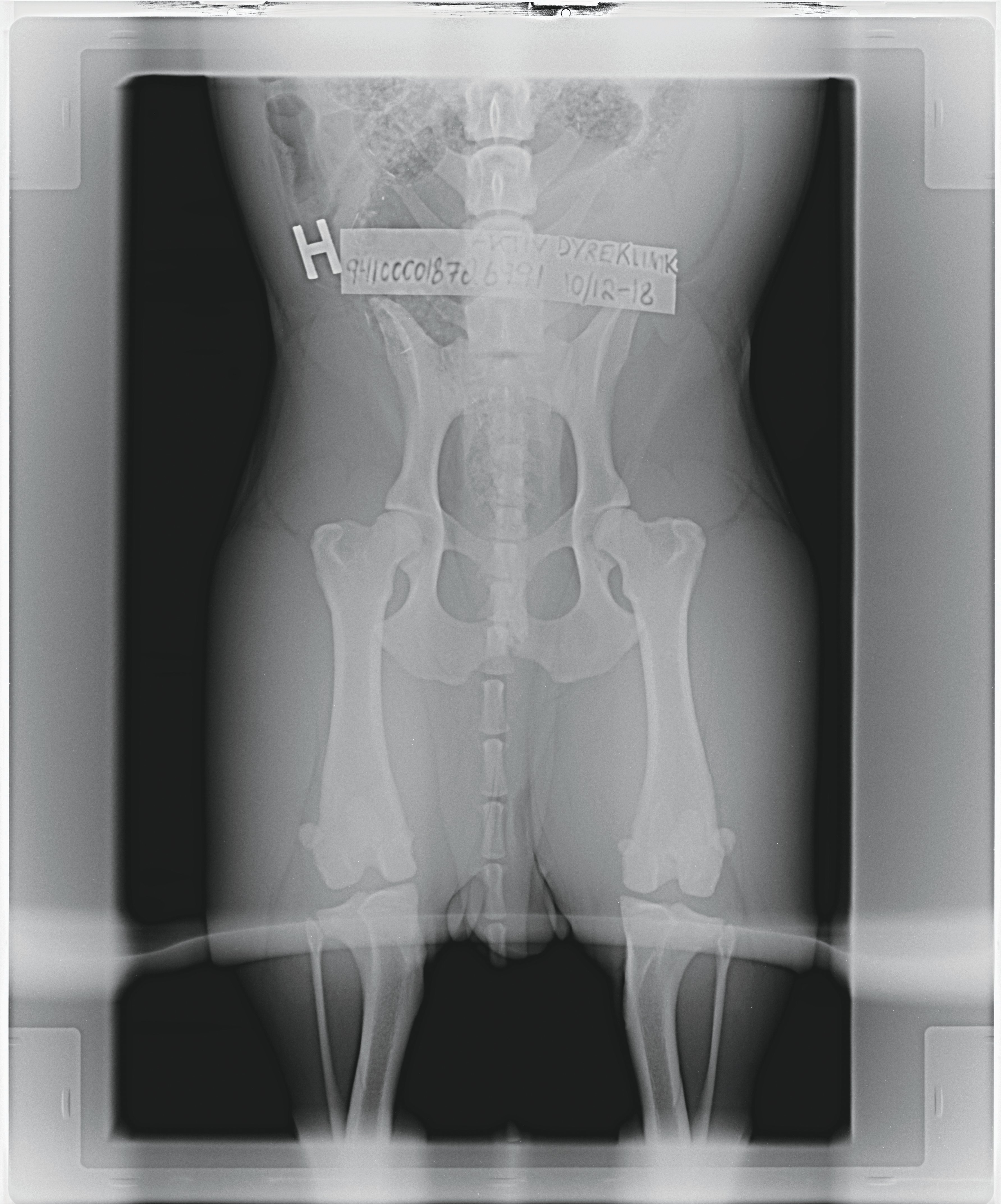
The FCI system is standard in countries that follow FCI regulations. The hips are evaluated on a ventrodorsal hip-extended radiograph. Grading (A–E) is based on several radiological criteria: joint congruence, the position of the femoral head in relation to the acetabulum, acetabular shape, any subluxation, and signs of osteoarthritis. The Norberg angle is used as a supportive quantitative measure of acetabular coverage (typically ≥100° for normal hips), but it is always assessed together with the other morphological findings and is not the sole basis for the grade.
The BVA/KC system in the United Kingdom also uses hip-extended radiographs, but the hips are scored point-by-point. Nine anatomical features are evaluated (including the Norberg angle, subluxation, and various acetabular and femoral structures), each scored from 0 to 6 per hip. The total score reflects hip quality, with lower scores indicating better hips. The Norberg angle is therefore only one of several sub-criteria within the BVA scheme. Like the FCI system, BVA assesses morphology and secondary changes rather than passive laxity.
The OFA system in the United States is also based on hip-extended radiography, but hips are graded through an overall morphological assessment: congruence between the femoral head and acetabulum, acetabular depth and shape, and any osteophytes or other arthritic changes. Three radiologists evaluate the images independently and classify hips as Excellent, Good, Fair, Borderline, Mild, Moderate or Severe. The Norberg angle is not an official element of OFA scoring. As with FCI and BVA, the OFA system assesses morphology and osteoarthritic changes but does not measure passive laxity.
PennHIP is the only established system that directly measures passive hip laxity by calculating a distraction index (DI). The method involves three standardised radiographic views taken under deep sedation or anaesthesia: a compression view, a distraction view, and a standard extended-hip view. The distraction view shows how easily the femoral head can be displaced relative to the acetabulum, and the DI is reported as a continuous value, where higher numbers indicate greater laxity and an increased risk of developing osteoarthritis.
PennHIP can be performed from 16 weeks of age and is the most accurate predictor of later osteoarthritis, but the technique requires specialised equipment and certification. For this reason, it is primarily used for individual risk assessment rather than as a population-level screening tool.
FCI, BVA and OFA are effective population-level screening tools because they reduce the prevalence of moderate and severe disease across a breed over many generations. However, they do not measure the underlying risk factor — passive hip laxity — and therefore provide limited information about an individual dog's genetic risk. PennHIP directly measures passive laxity and is therefore the most precise method for assessing an individual dog's hereditary risk of HD, but it is not suitable as a broad, mandatory screening tool because the technique is more demanding and less widely available.
Clinical Relevance
Large and heavy breeds often develop earlier and more pronounced symptoms than smaller and lighter breeds. Muscular breeds may have significant laxity that is not visible on hip-extended radiographs but still contributes to osteoarthritis later in life. A "normal" HD grade therefore mainly reflects the hip status at the moment the radiograph was taken, not necessarily long-term stability or function.
Common Misconceptions
- An FCI A or B grade does not guarantee stable hips — it only means no visible secondary changes were detected.
- Conventional HD radiography (FCI, BVA and OFA) does not show joint function during movement — it only represents a static position.
- Sedation is not just for comfort — it reduces muscle tension that may otherwise mask instability.
- Breeding from dogs with normal hip grades does not eliminate genetic predisposition to laxity, but it does reduce the prevalence of severe HD within a population.
References
Scientific literature
- Smith GK et al. Evaluation of passive hip laxity and DJD in dogs. JAVMA, 1997–1998.
- Lust G et al. Developmental hip dysplasia: radiographic and pathologic features. Vet Clin North Am Small Anim Pract, 1992.
- Kealy RD et al. Effects of restricted feeding on hip dysplasia and DJD. JAVMA, 1997 & 2002.
- Powers MY et al. Comparison of PennHIP DI and OFA scoring. Vet Surg, 2010.
- Culp WTN et al. Canine hip dysplasia: current concepts and controversies. Animals, 2021.
System sources
- FCI Hip Dysplasia Grading Protocol
- BVA/KC Hip Dysplasia Scheme Manual
- OFA Radiographic Procedures & Guidelines
- PennHIP Scientific Overview (University of Pennsylvania)